Frequent Diagnoses
Sudden vertigo attacks are not without danger, for example, if they occur while driving or lead to a fall. The fear associated therewith, like acrophobia, can become independent and lead to long-lasting symptoms: Phobic postural vertigo is particularly common as the sole cause, or as secondary cause of dizziness – but not vertigo sensu strictiori. In the second most frequent form of vertigo, the benign positional vertigo [BPV], that may follow attrition or light head concussions, is caused by broken small crystals of calcium carbonate (lime) in the inner ear that now float within the semicircular canals of the vestibular system: At each change of position they sink to the deepest point and the liquid is then accelerated in the semicircular canal: The patient experiences short, violent attacks of rotational vertigo. With a simple positioning maneuver, these lime particles are flooding out of the semicircular canals and so the symptoms are relieved in up to 90 %.
Also, unilateral or bilateral loss of the vestibular organs, inflammatory changes of the vestibular nerve as well as Meniere’s disease always lead to vertigo. Less frequently but not less importantly, vertigo-migraine, neuro-degenerative diseases, and especially circulatory disorders of the brain stem or cerebellum must be seen by the neurologist: If dizziness/vertigo is accompanied by visual, speech, or movement disorders of the arms and legs, this is an emergency. A too high or too low blood pressure often leads to dizziness, lightheadedness, fainting or syncope.
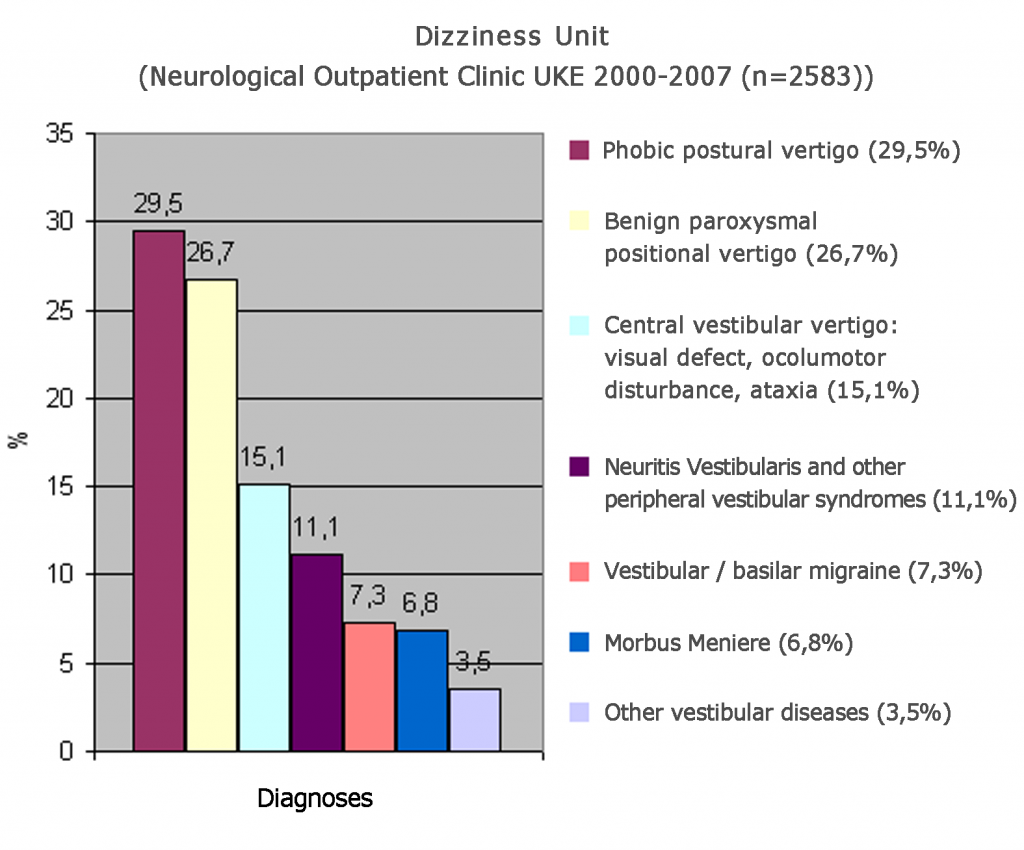
An overview of the years 2000 – 2007 from the Dizziness Unit of the Neurology Clinic at the University Hospital Hamburg is shown in Fig.1.
At old age, dizziness and unsteadiness are often seen as “normal” part of aging. That this is not correct, and is demonstrated by a variety of studies in this area.Doctor Klaus Jahn and coauthors most recently reported in the “German Aerzteblatt” (2015; 112: 387-93) a comprehensive literature review about the age distribution of special vertgo diagnoses and also data of the “German Vertigo Centre Munich” (n=500 consecutive patients). There, the incidence of dizziness syndromes in very elderly patients (> 80years) and young patients (<40years) were compared.
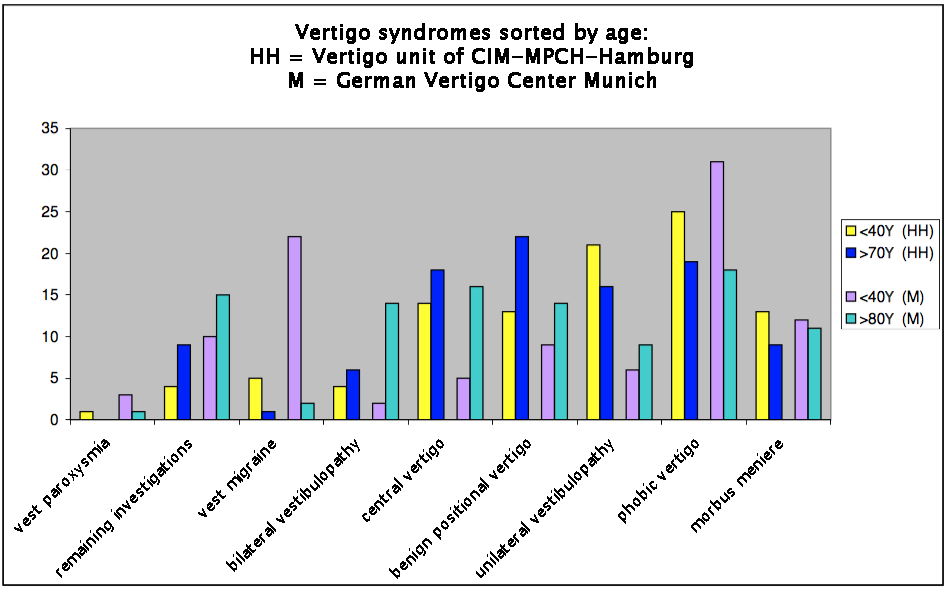
In Fig.2 we have compared their results with our own findings from the University neurology clinic and the CIM-MPCH from the past 5 years (n = 562; “old”> 70years, “young” <40years).
Diagnostic Tests
Considerations in the neuro-ophthalmological / neuro-otologic examination:
Recording of: spontaneous, gaze, fixational, position, or positional nystagmus. Signs of central vestibular disorders and/or other neurological symptoms/signs that point to a possibly central disorder. Subsequently, examination of the oculomotor and the vestibular system: Examination of the eye position / motility (velocity, acceleration, latency), incl. cover test. Smooth pursuit eye movements, and suppression of the vestibular ocular reflex during smooth head movements and the optokinetic reflex movements. Recording of fast eye movements (saccades) under various conditions. Clinical testing of peripheral vestibular functions and the vestibulo-ocular reflex (VOR) by rapid head rotation with/without fixation of a stationary point. Investigation under socalled Frenzel glasses. Blind stand (RombergTrial), blind walking on the spot (UnterbergerTrial). Investigations of balance and in the oculomotor laboratory with infrared electro-oculographic, and electro-nystagmographic recordings, incl. calorisation, and rotarational tests; click-evoked vestibular- neck-potentials, as well as -eyemuscle-potentials; neurosonology.